This is the second post in our series, “Raising the Bar for Indian Healthcare”, which highlights the challenges and opportunities facing India’s healthcare delivery system. In this post, we discuss the state of PPPs in the health sector, and the need for greater evidence on performance and enablers.
Since Government’s endorsement almost 15 years ago as a potential solution to deficient health service delivery, healthcare public-private partnerships (PPPs) have proliferated across India. They represent a rare form of public-private collaboration in a system dominated by private provision, but inhibited by considerable distrust between the two sectors. In effect, public-private engagement for service delivery in India’s health system hardly moves beyond the micro-level realm of PPP transactions. More recently, however, government-sponsored insurance schemes such as PM-JAY are purchasing insurance-related services from private third-party administrators and health services from private hospitals, and represent a bold step forward in public-private engagement. In this post, we focus on PPP models oriented toward expanding service delivery in which state health agencies contract private entities to build and operate facilities or manage services heretofore delivered through the public delivery system. Despite the proliferation of these transactions, little is known about their scope and impacts.
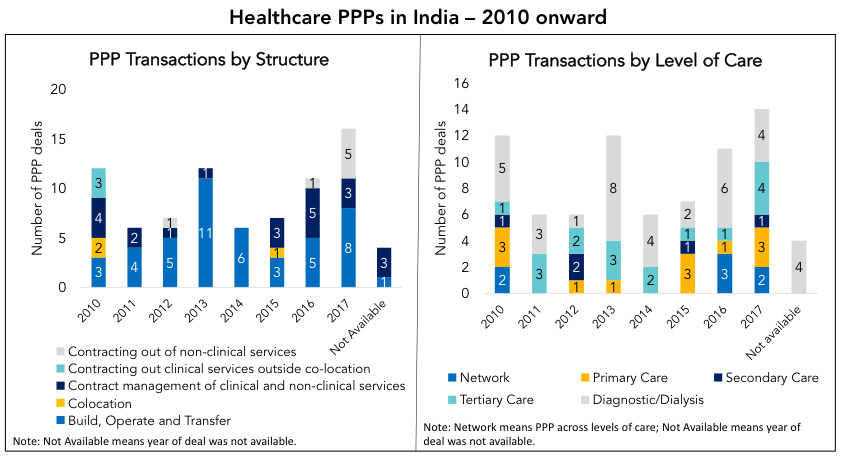
We began analyzing the state of healthcare PPPs in India about a year ago, and quickly found that the evidence-base is thin. In India, states are constitutionally responsible for publicly-financed health service delivery. Our analysis of multiple tender documents, newspaper articles, reports and websites of state PPP cells reveals that over the past decade, state governments across India have primarily focused on infrastructure PPPs. A growing number of states are experimenting with service delivery PPPs . Many of these involve the contracting out of select clinical and non-clinical services, such as diagnostic services (ex: Bihar, Himachal Pradesh) and dialysis services (ex: Delhi, Andhra Pradesh). Some states, such as Karnataka, Meghalaya and Arunachal Pradesh, have outsourced management of some primary care clinics to NGOs. To a lesser extent, states have or are experimenting with contracting out hospital management and service delivery (see examples here and here). Data on the actual number of ongoing PPPs is difficult to obtain or validate.
The impact of these PPPs in terms of quality of care, costs and alignment with public priorities is largely unknown. Some diagnostic and dialysis PPPs have reported positive performance (see here and here), possibly because their narrow scope makes them relatively easier to design, tender, manage and monitor. One model that has widely been panned as a failure is the “land for beds model”, in which land is leased to a private partner to build and operate a hospital at little or no cost, in exchange for meeting specific conditions, usually including designating a share of beds to the poor. A troubled joint venture between the Delhi Government and Apollo Group exemplifies the challenges of this approach. Amazingly, this form of PPP remains under consideration in other states.
Anecdotal evidence suggests that some private operators faced insolvency in part due to late payments from government agencies. Further, while PPPs are often employed to fill gaps in access and quality that the public sector cannot address through its own resources, contracts often lack critical details: performance indicators, accountability frameworks and standard operating procedures are generally missing. As elsewhere, the public sector’s low capacity for contract management in India may be the Achilles heel of PPPs.
The lack of good quality information and data on specific healthcare PPPs in India is concerning. States across India are moving forward with this agenda (see here and here), and many interesting engagements are underway; yet there is little to no rigorous evaluation or even monitoring of these initiatives. Much of the evidence to date is drawn from “light touch” case studies that often appear promotional in nature. Little is known about impacts, lessons learned, and how starting conditions and government and contractor capacities contributed to performance.
As a result, states are left largely to operate in the dark, with limited knowledge of what has worked elsewhere in India, and why. The often ad hoc nature of PPP transactions leaves them vulnerable to repeat past failures, and unable to systematically learn from successes. More and better information and analysis are needed to inform state and national PPP policies so that governments can move this agenda forward in a more informed way. Until then, we can’t be sure why some PPPs succeed while others fail.
Check out other posts in this series below:
Let Managers Manage: Raising Indian Public Hospital Performance